In a nutshell . . . .
This page introduces you to the third of the six ideas that give life to the Therapeutic Milieu, Respect for inherent human dignity. The Universal Declaration of Human Rights (United Nations 1948) declares that "recognition of the inherent dignity and of the equal and inalienable rights of all members of the human family is the foundation of freedom, justice and peace in the world".
In this page you will read about how inherent human dignity is understood in Careful Nursing, and that inherent dignity can never be lost or taken away. Although human dignity is considered a core nursing value – if not the core nursing value – its recognition and respect in practice is sometimes overlooked.
Professional nursing codes of conduct and ethics are reviewed and noted to vary in their attention to the importance of respect for human dignity. The American Nurses Association code of ethics seems to be the only code that recognises inherent human dignity. You will find that, generally, there is a range of views on the importance of human dignity, with some bioethicists saying that human dignity is not a useful idea.
Also reviewed are the vitally important acquired types of human dignity, such as dignities of personal identity; these are types of dignity that can be lost or taken away. Dignities of personal identity become especially vulnerable during acute and chronic illness and in older and disabled persons.
Dignity checks are suggested and dignity related implications are given for practice.
Introduction
Respect for inherent human dignity is the third concept of the Therapeutic Milieu because, in metaphysical terms, the inner spirituality of persons mirrors their likeness to Infinite Transcendent Reality in life processes, a philosophical principle of Careful Nursing. As persons, every human individual is distinctive and unique yet all share equally and unconditionally in inherent dignity; all are of inherent value and worth. Inherent dignity is recognised as a unifying concept and the highest human value.
Careful Nursing's philosophy of the human person also recognises in the individual distinctiveness of human persons the many acquired human dignities which are integral to human health and flourishing. Acquired human dignities come into being primarily in the outward life of body and senses as unitary human persons engage in relationships with others and in self-care.
When Careful Nursing was initially constructed as a philosophy and professional practice model human dignity was addressed only in the philosophy. It was assumed that through the philosophy, recognition of and respect for human dignity would be fully infused into the practice model.
Further review of literature, experience in practice and reflection highlighted the importance of ensuring that, to every possible extent, recognition and respect for human dignity was embedded concretely in practice. It is widely evident that although human dignity is a core nursing value – if not the core nursing value – its recognition and respect can be easily overlooked (Baillie & Gallagher 2012, Francis 2013).
In addition, in clinical practice it is logical that recognition of human dignity must be considered equally with respect for human dignity; human dignity must be recognised before it can be respected.
Baillie and Gallagher (2012) found that nurses' use of visual metaphors helped them to recognise human dignity and thereby respect it in practice situations. Munoz et al. (2017) emphasise that in clinical practice settings dignity is an inter-relational and personally experienced concept; they demonstrated that in relation to learning to respect human dignity in practice, nursing students' greatest desire was to recognise dignity by seeing it modelled by nurses in practice.
Divergent views about human dignityBefore focusing on human dignity in Careful Nursing, it is important to be aware that philosophical underpinnings and value accorded to human dignity vary and are widely contested (Riley & Bos), and that there is also disagreement about the nature of respect and self-respect (Dillon 2016).
Universal Declaration of Human Rights
The emergence of human dignity as an important concept is relatively recent and gained prominence particularly with the formulation of the Universal Declaration of Human Rights (United Nations 1948). This declaration boldly asserts in the first statement of its preamble that:
'recognition of the inherent dignity and of the equal and inalienable rights of all members of the human family is the foundation of freedom, justice and peace in the world'.
However, this declaration as a whole has been interpreted in a range of ways some of which do not recognise that all human persons have inherent dignity (Glendon 1999). The nature of human dignity and agreement about what it means has proved elusive. While some bioethicist support human dignity (Schroeder 2008) others argue that it is not a useful idea (Macklin 2003) and far too subjective to provide practical guidance (Cochrane 2009).
The philosophy of Immanuel Kant is often drawn on to argue that inherent dignity is conditional on persons' actual capacity to reason (Shell 2008). When persons do not have this capacity, for example, a child still developing capacity, a person in a seemingly irreversible coma or an elderly confused person, their human dignity may be questioned.
Nurses' professional codes of conduct and ethics
As nurses we are guided by our code of professional conduct and ethics. However professional codes differ internationally. Only the American Nurses Association (2015) Code of Ethics for Nurses mentions inherent dignity:
'The nurse practices with compassion and respect for the inherent dignity, worth, and unique attributes of every person' (p. 1).
The Nursing and Midwifery Board of Ireland Code of Professional Conduct and Ethics (2014) refers prominently to respect for the dignity of the person, citing the Universal Declaration reference to inherent dignity.
But other nursing codes of ethics do not mention inherent dignity. The Canadian Nurses Association (2008) Code of Ethics for Professional Nurses states that nurses must uphold and maintain the dignity of all persons. Both the International Council of Nurses (2012) Code of Ethics for Nurses and the United Kingdom Nursing and Midwifery Council (2011) code of standards, conduct and ethics refer only secondarily to respecting the dignity of people
Implications in practice settings
In any nursing practice setting it is likely that there will be differing understandings of respect for human dignity and that some understandings will not be consistent with the Careful Nursing understanding. It is important to be aware that contrasting views about human dignity will seek, often in subtle ways, to undermine the Careful Nursing view.
It is also evident in the literature that, in grappling with our fallible human nature, we can easily inadvertently overlook the dignity of the people we care for (Baillie & Gallagher 2012, Hayter 2013, Kagan 2017) as well as our own dignity and the dignity of colleagues (Moore et al. 2013). Baillie and Gallagher found that when nurses are prompted to think in retrospect about their practice they are able to identify times when they have not thought about or respected patients' dignity.
Human dignity in Careful NursingRecognition of and respect for inherent human dignity
As indicated in the Careful Nursing philosophy, respect for inherent human dignity is founded in the understanding that every human person in their essential being is ordered towards goodness and human flourishing. Therefore, every human person, without exception, has inherent dignity; is of the greatest value and worth. Inherent human dignity is recognised in contemporary bioethics (Schroeder 2008) healthcare generally (Nordenfelt 2004) and nursing (American Nurses Association 2015).
In a philosophical analysis of human dignity, Lebech (2009, p. 291) concludes that dignity is:
'the fundamental value of the human being' and that all human persons are equal in inherent dignity.
Accordingly, inherent dignity is a unifying value. Awareness of the inherent dignity of ourselves and all human persons brings us together equally to embrace human dignity in relationship with one another.
As a concept of the therapeutic milieu, inherent human dignity brings us into practical relationship with our own inherent dignity and that of one another, patients, and all involved in patients' care. Recognition and respect for inherent human dignity becomes a thread that we knit consciously into the attitudes and actions through which we implement all the practice model concepts. We are guided frankly to actualise inherent human dignity as a value, unconditionally and without exception, irrespective of our own, patients', colleagues' and others personal characteristics, social circumstances, attitudes or actions.

Because inherent human dignity emerges in the essential being of human persons' it can never be lost or taken away. However, when persons do not recognise their own inherent dignity or the inherent dignity of others it can appear to be lost; when persons' inherent dignity is not respected it can feel to them that it has been taken away.
Recognition of and respect for acquired human dignity
All human persons have acquired dignities related to their individual identity and attributes which merge with their inherent dignity (Nordenfelt 2004, Schroeder, 2010). Acquired dignities can depend on merit, for example, high social standing, exceptional leadership or outstanding skill. Acquired dignity can also accrue from gracious comportment or moral stature. Acquired dignities must be recognised and respected to every possible extent. All persons can aspire to these types of dignity but only some persons can acquire them, and these types of dignity can also be lost.
Further, all human persons have an acquired range of personal dignities of identity, indicating their sense of integrity of body and mind, and also usually their self-image (Nordenfelt, 2004). Dignities of identity reflect who each person is as a distinctive, autonomous human being with a cultural background, personal aspirations and desire for relationships with others. For example, a sense of integrity will include dignities concerning personal appearance, privacy and ability to engage in self-care. Dignities of identity can be acquired in different ways, for example, through culture, nationality, occupation, or special interest; these dignities can be changed or discarded.
Nordenfelt (2004) observes that most people respect their own identity, that is, have self-respect. But this respect can be easily diminished or destroyed. Nordenfelt (2009) emphasises the significance this type of personal dignity can have during illness, injury and the aging process, conditions which can strip affected people of this dignity, for example, by physical disfigurement or disability.
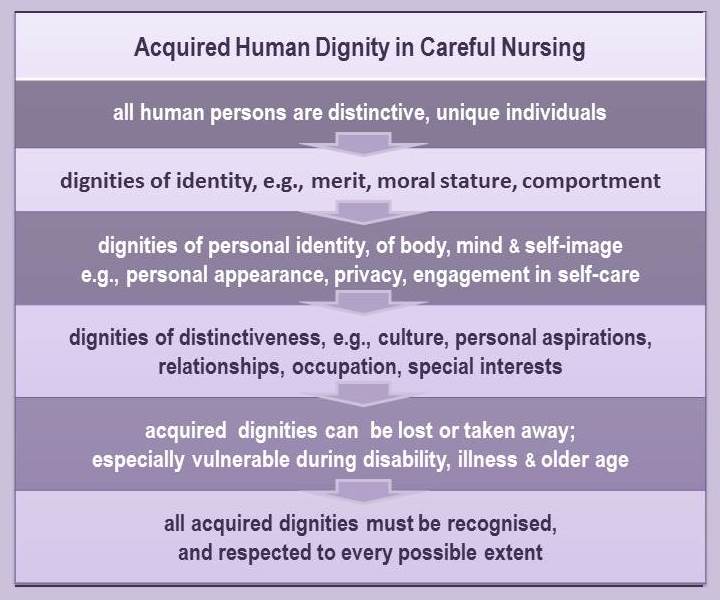
The most significant characteristic of acquired human dignities, especially dignities of identity, is that they are integral in human relationships (Munoz et al. 2017) and their preservation depends on personal experience of their recognition and respect. Acquired dignities of identity can be lost or taken away. During times of acute illness acquired dignities can become very fragile and be profoundly affected by how people, especially elderly people, are cared for (Nordenfelt 2009, Kagan 2017); dignity can be respected and supported by attentive, sensitive care but can be destroyed by humiliating, thoughtless or harsh attitudes or actions of nurses and their assistants. The truth of this is borne out by reports of disrespectful and damaging nursing practice (Milton 2011, Francis 2013, O'Ferrall, 2013).
Implications for nursing practice
Unconditional respect for inherent human dignity, and respect for acquired human dignities of ourselves, our patients, colleagues and assistants to every possible extent are central in creating a therapeutic milieu.
Respect for human dignity brings ethics into the professional practice model. Thus, every aspect of our practice is guided by recognition of the philosophical principle, the nature and inherent dignity of the human person. Varieties of acquired dignity as they pertain to the people we care for and to ourselves alert us to the many ways in which we are ethically responsible to respect human dignity in our practice.
Recognising and respecting our human dignity as professional nurses
It is important for us to recognize and respect our own dignity as professional nurses, an aspect of our personal dignity. It is also important for each of us to reflect on our personal understanding of dignity in relation to our professional code of ethics. Recognition of and respect for our own dignity will enable us to fully recognise and respect the dignity of persons we care for and persons we work with (Glendon 1999).
Doing a dignity check! We can begin by tuning in to our inward life (facilitated by being in the habit of spending at least five minutes in 'stillness' each day). Then let us ask ourselves:
► How do we perceive and experience our inherent dignity?
► How does our experience of inherent dignity influence our practice?
► How do we recognise inherent dignity in one another?
► Which acquired dignities are important to us? Do we respect them?
► How is our self-respect?
►Do we recognise which dignities of identities are important to our colleagues? Do we recognize and respect them?
Reading alert! The extensive literature on bullying in nursing (Vessey et al., 2011) suggests that this disruptive relational behaviour stems from our lack of sensitivity to our own personal and professional dignity and self-respect, and that of colleagues and assistants.
► We can also ask ourselves where we and our colleagues are in aspiring to dignity of merit.
► How might we be working toward being especially accomplished in some way? Are some of us there? How do we acknowledge and respect our achievements?
► How are we with dignity as comportment? How gracious and respectful are we generally?
Our recognition and respect for these dignities in ourselves will influence the quality of the therapeutic milieu that we create.
Recognising and respecting the dignity of people we care for
Guided by our philosophy, we are responsible to recognize and respect the inherent dignity, the fundamental value of every person we care for. Again, our five minutes of 'stillness' each day will support us in this.
Our nursing assessments and relational continuity with patients alert and sensitize us to their inherent dignity and acquired dignities, especially dignities of identity. Research shows that when patients dignities of identities are not respected they experience many violations and losses of dignity, for example, being treated as objects, being left with obvious personal needs not attended to, feeling as though they are disgusting, being condescended to and being discriminated against (Jacobson, 2009; Baillie, 2009). Older people are especially vulnerable to such violations and losses (Nordenfelt 2009, Kagan 2017).
Reading alert! Locate and read this article: 'Digging deeper into dignity' by Sarah H. Kagan published in Geriatric Nursing, 38, 2017, 460-463. Pay close attention to the case study introduced in the first paragraph and continued in the last five paragraphs.
Reflect on how the nurse, Mr. Edison, recognised and respected the dignity of 97-year old Mrs. Thane admitted to an acute care hospital with pneumonia.
Reflect on how you would have cared for Mrs. Thane and how closely your care would have approximated that of her nurse, Mr. Edison.
Note that Kagan observes 'how seemingly small or apparently insignificant elements within nursing care for older people generally represent consequential actions supported by' competence in caring for older persons, appreciation of differences perspectives between generations, or both (p462.).
Research shows that health care providers, including nurses, can fail to recognize and respect obvious patient dignities of identities and become defensive about this; "we don't do that", we would never do that" (Baillie & Gallagher, 2012, p.46). Such lack of recognition is obviously unacceptable. At the same time, it is an example of a common human fallibility that we are all very capable of, especially when we are anxious, tired, and practicing in stressful and short-staffed situations.
Further, when we are aware of our failures to respect patients' dignity, we can still find it difficult to respond appropriately, for example, when we encounter someone who treats us in a snide, patronizing or angry way, or someone who is confused, acts abusively or is frequently incontinent.
In such situations it is important that we draw on our capacity to remain calm. When we are calm we can be become aware of our inherent dignity and self-respect. In turn, we can more easily recognise patients' inherent dignity and dignities of identity. Our capacity to embrace human dignity in ourselves and others depends on and is supported by our practice of stillness each day for at least five minutes.
Doing a dignity check! We can plan to have a 'dignity check' on a regular basis. This could be done briefly every so often before or after shift handover. Or it could be done from time to time at a stand-up huddle (Shermont et al, 2008). Questions might include:
► How are we doing with awareness of patients' inherent dignity?
► What are our patients' dignities of identity?
► Are there patients whose dignity we have difficulty recognising and respecting?
► Are there things that we need to do to enhance our recognition of and respect for patients' dignity?
Creating physical surroundings which respect dignity
We may need to take time to review whether patients' physical milieu itself is therapeutic in terms of respect for human dignity. Research has identified the importance of patient's physical environment, especially the cleanliness of toilets, bathroom areas and the use of doors or privacy curtains and provision of clothing to respect patients' dignity (Jacobson, 2009; Baillie, 2009).
Human dignity 'I will' statements
Sit quietly in a chair, close your eyes and take a moment to relax and recall your experience of stillness. Bring to mind your practice experiences over the past month.
On a scale of 1 to 10, how do you rate your level of recognition and respect for your own dignity?
On a scale of 1 to 10, how do you rate your level of recognition and respect for patients' dignity?
On a scale of 1 to 10, how do you rate your level of recognition and respect for colleagues' dignity?
 Based on your assessment of your current level of recognition and respect of your own, patients' and colleagues' inherent dignity and acquired dignities, decide what you will do to further develop in yourself this enduring personal quality in order to contribute further to creating a culture of dignity in the therapeutic milieu in your practice setting?
Based on your assessment of your current level of recognition and respect of your own, patients' and colleagues' inherent dignity and acquired dignities, decide what you will do to further develop in yourself this enduring personal quality in order to contribute further to creating a culture of dignity in the therapeutic milieu in your practice setting?
Examples of human dignity 'I will' statements:
. . . think each day of myself, patients and colleagues as being of equal worth
. . . ensure that patients' preferred name is used to address them
. . . . . . . . . . . . . . . . . . . . . . . . .respect patients' wishes about how they want to be care for
. . . . . . . . . . . . . . . . . . . . . . . . .protect patients' privacy during self-care activities
References
American Nurses Association (2015) Code of ethics for nurses with interpretive statements. American Nurses Association, Silver Spring, MD.
Baillie L & Gallagher A (2012). Raising awareness of patient dignity. Nursing Standard, 27(5), 44-49.
Canadian Nurses Association (2008) Code of Ethics for Professional Nurseshttp://www.cna-aiic.ca/en/on-the-issues/best-nursing/nursing-ethics
Cochrane A (2009) Undignified bioethics. Bioethics, 24, 234-241.
Dillon RS (2016). "Respect", The Stanford Encyclopedia of Philosophy (Winter Edition), Edward N. Zalta (d.), URL = <https://plato.stanford.edu/archives/win2016/entries/respect/>.
Francis R (2013) Report of the Mid Staffordshire NHS Foundation Trust public inquiry. Controller of Her Majesty's Stationery Office. Contains public sector information licensed under the Open Government Licence v2.0, London.
Glendon MA (1999) Foundations of human rights: The unfinished business. The American Journal of Jurisprudence, 44, 1–14.
Hayter M (2013) The UK Francis Report: the key messages for nursing. Editorial. Journal of Advanced Nursing, 69, e1-e3.
International Council of Nurses (2012) Code of Ethics for Nurses. http://www.icn.ch/about-icn/code-of-ethics-for-nurses/
Jacobson N (2009) A taxonomy of dignity: a grounded theory. BMC International Health and Human Rights, 9, 9.
Kagan SH (2017) Digging deeper into dignity. Geriatric Nursing, 38, 460-463.
Lebech M (2009) On the Problem of Human Dignity. Wurzburg: Verlag Konigshausen & Newmann.
Macklin R. (2003) Dignity is a useless concept. British Medical Journal, 327 (7429), 1419-1420.
Milton C L (2011) An ethical exploration of quality and safety initiatives in nurse practice. Nursing Science Quarterly 24, 107-110.
Moore LW, Leahy C, Sublett C & Lanig H (2013) Understanding nurse-to-nurse relationships and their impact on work environments. Medsurg Nursing, 22, 172-179.
Munoz S-A, Macaden L, Kyle R & Webster E (2017) Revealing student nurses' perceptions of human dignity through curriculum co-design. Social Science and Medicine 174, 1-8.
Nordenfelt L (2004) The varieties of dignity. Health Care Analysis, 12(2), 69-80.
Nordenfelt L (2009)) The concept of dignity. In L Nordenfelt (Ed.) Dignity in Care for Older People (26-53): Chichester UK: Wiley-Blackwell
Nursing and Midwifery Board of Ireland (2014) Code of Professional Conduct and Ethics http://www.nursingboard.ie/en/code/new-code.aspx
Nursing and Midwifery Council (United Kingdom) (2011) The Code http://www.nmc-uk.org/Publications/Standards/The-code/Introduction/
Riley S & Bos G (2017) Human Dignity. Internet Encyclopedia of Philosophy. http://www.iep.utm.edu/hum-dign/
O'Ferrall F (2013) Crisis in caring: An evidence-based response. Studies, 102 (407), 324-335.
Schroeder D (2010) Dignity: One, two, three, four, five, still counting. Cambridge Quarterly of Healthcare Ethics, 19, 118-125.
Shell SM (2008). Kant's concept of human dignity as a resource for bioethics. Human Dignity and Bioethics: Essays Commissioned by the President's Council on Bioethicshttps://bioethicsarchive.georgetown.edu/pcbe/reports/human_dignity/chapter13.html
Shermont H, Mahoney J, Krepcio D, Baccari S, Powers D & Yusah A (2008) Meeting of the minds. Nursing Management, 39(8), 38-40, 42-44.
United Nations (1948) Universal Declaration of Human Rights. http://www.un.org/en/documents/udhr/
Vessey JA, DeMarco RF, & DiFazio RL (2011) Bullying, harassment, and horizontal violence in the nursing workforce. In A Debiesette & J Vessey Annual Review of Nursing Research: Springer Publishing Company, New York, NY.
Therese C. Meehan © July 2020