PPMs emerged in the 1990s, defined as a "system (structure, process, and values) that supports registered nurse control over the delivery of nursing care and the environment in which care is delivered" (Hoffart & Woods, 1996, p. 354).
Note that Careful Nursing includes a professional practice model (PPM). Careful Nursing is both a philosophy and a PPM – the two are integral and cannot be separated. So to make this clear, the right way to refer to the PPM is to say, "the PPM of Careful Nursing", and not the Careful Nursing PPM.
PPMs developed further with development of the Magnet Recognition Program®(American Nurses Credentialing Center (2014), widely recognised as a benchmark for excellent nursing practice. Thirty-eight published PPMs were identified and reviewed by Slatyer et al., in 2016, one of which was the Careful Nursing PPM.
PPMs differ from conceptual models of nursing in that their primary aim is not the development of nursing science as such. Rather, PPMs are theoretical frameworks based on actual professional nursing practice judged to be of a high standard. Then when PPPs have been implemented and tested in practice can they be used to advance nursing science.
PPPs also differ from conceptual models of nursing in that their central, stabilising element is values, that is, the professional belief system of nurses that informs their education and underlies their practice (Hoffart & Woods, 1996).
Without values other elements of PPMs, such as professional relationships, the patient care delivery system, and the management approach, are left without focus and coherence. Values, along with the corresponding characteristics, attitudes, and activities that they generate are considered the mainstay of professional practice.
In their analysis of 38 existing PPMs, Slatyer et al., (2016) describe PPMs as depicting nursing values. However, while Slatyer et al., describe key PPM concepts which could be considered nursing values, they emphasise that most PPMs adopt the values of the healthcare organisation in which nurses are employed rather than nursing values per se.
PPMs in which nursing values are replaced with the values of healthcare organisations in which nurses are employed is inconsistent with Hoffart and Woods (1996) emphasis on the importance of nursing values for PPMs.
Slatyer et al., (2016) propose that nursing's adoption of healthcare organisational values ensures that nursing is thoroughly merged with the organisational culture in which nurses are employed. However, unless nurses are actually governing a healthcare organisational culture, there is no assurance that nursing values will be recognised, prioritised, and acted upon.
The professional practice model of Careful Nursing
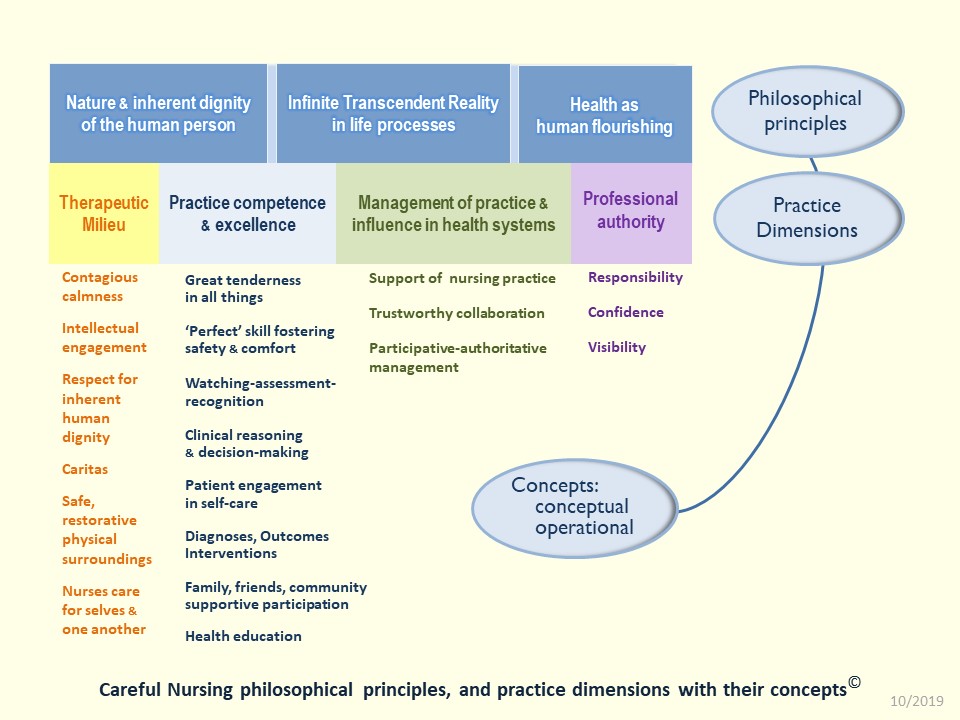
Principles and concepts in themselves are not regarded as values. However, the three Careful Nursing philosophical principles, twenty PPM concepts and their sub-principles and sub-concepts are regarded as values because they motivate the practice of Careful Nursing. The philosophical principles always inform the PPM, whether or not they are shown in any given PPM diagram.
A linear diagram of the PPM with its philosophical principles:
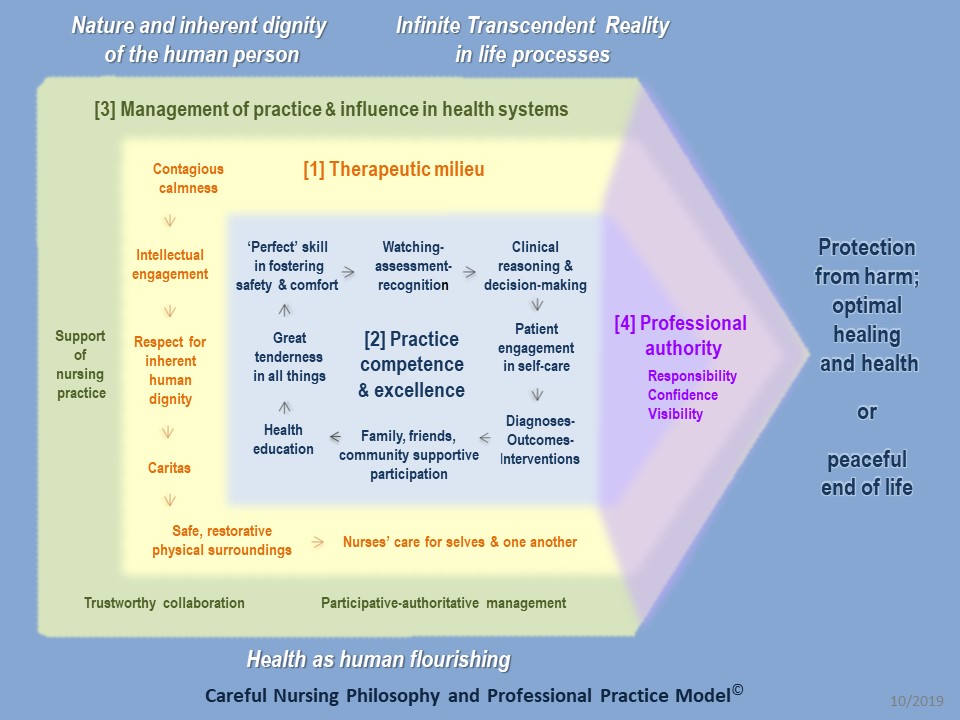
A practice oriented diagram of the PPM with its philosophical principles:
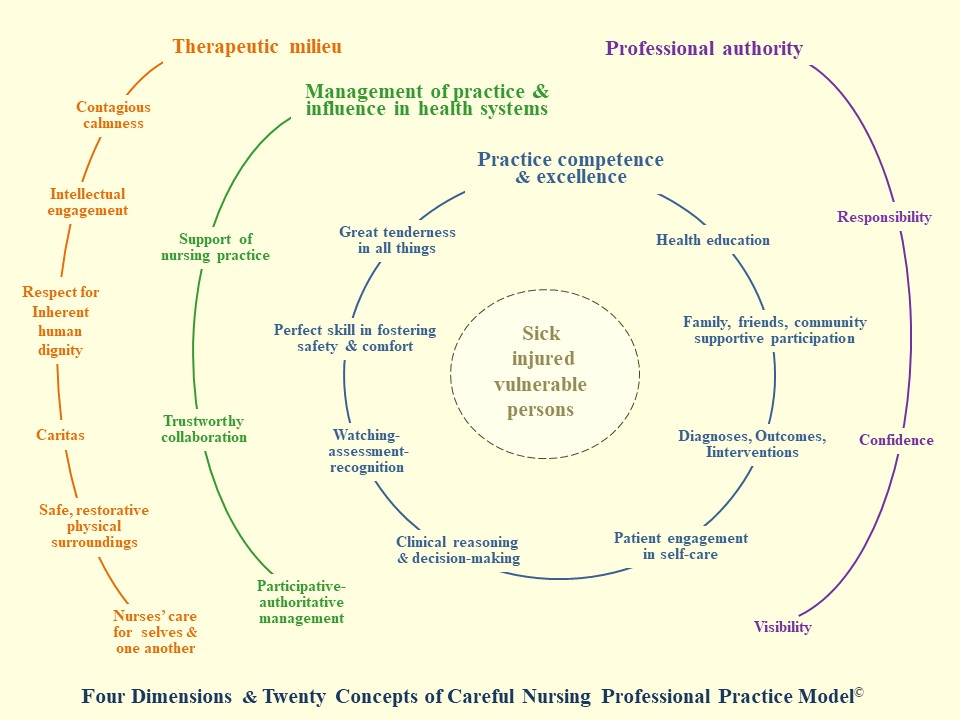
Circular diagram of the PPM (philosophical principles not shown):
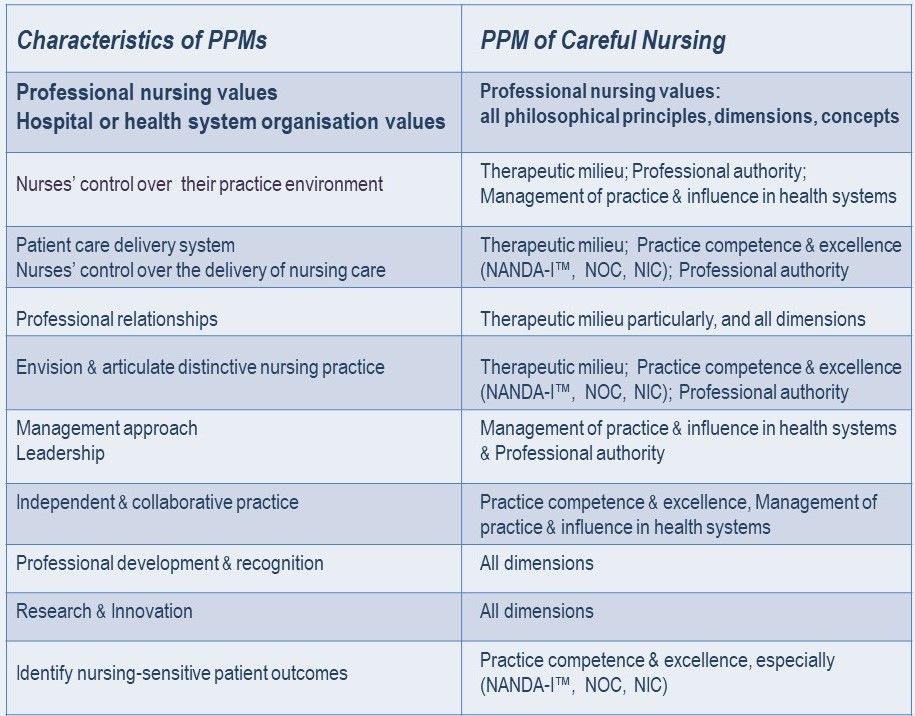
The Table below shows the characteristics of PPMs in relation to the dimensions of the PPM of Careful Nursing in which they are mainly reflected:
Professional nursing values
Nursing codes of ethics are considered to be the most accurate summary of the profession's core values, values that are required to guide all nursing education, practice, and research. These values are widely identified and discussed in the nursing literature. Careful Nursing values are consistent with the profession's core values. Here we will focus in on Careful Nursing values.
Careful Nursing values
Stein's value theory used to understand Careful Nursing values
Because values have such a significant influence on the quality of our nursing practice it's important that we know what values are and how they work in our practice. In Careful Nursing we base our understanding of values and how they work in our practice on Edith Stein's value theory (Stein, 1921/1989; Lebech, 2015).
To begin with two important points:
► Strictly speaking, what we commonly call values are attitudes of value; attitudes associated with the actual value itself. For example, justice is a value; fairness, respect and honesty are some of the many value attitudes of justice.
► In nursing we almost always think of values as being positive because our professional codes of conduct and ethics are built on our professional values, which are naturally positive.
However, values can also be negative. Consider the following Figure:
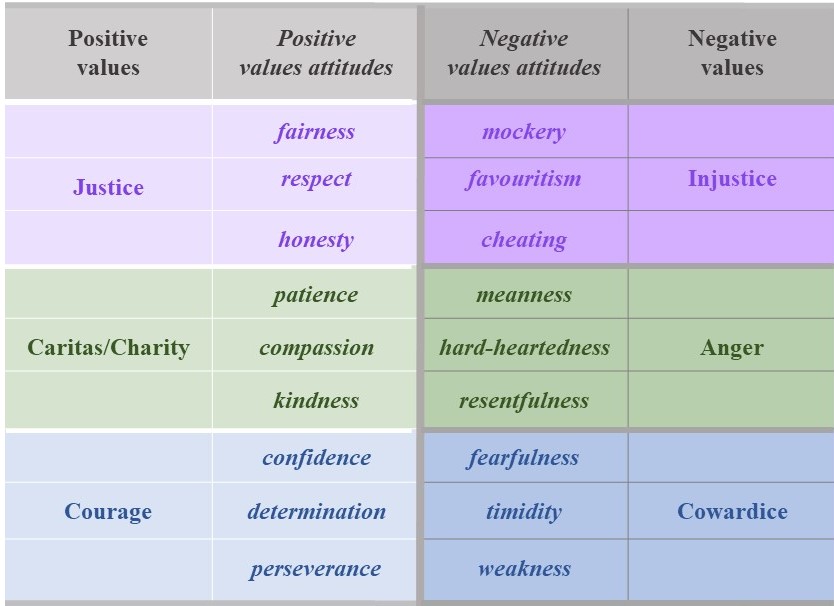
On the left of the Figure you see examples of positive values with some of their many value attitudes. These are values and value attitudes we are familiar with because they are included in our professional codes of conduct and ethics.
On the right you see examples of negative values with some of their many value attitudes. These are values and value attitudes we are likely to be somewhat familiar with even though they are negative. Why do we need to be aware of negative values?
All human beings, including ourselves, are plagued by human weaknesses. That is, we as nurses are all susceptible to implementing negative values in our practice. Think about reports of inquiries into harmful nursing care, such as the Mid Staffordshire report and the Leas Cross report. Think about the terrible problem we have with bullying in nursing.
Why is it that we can sometimes implement negative values?
We can find negative values arising in our practice if we don't remain strongly committed to implementing our positive professional values. Commitment to our professional values can weaken insidiously over time for various personal or circumstantial reasons. Or, our normally strong commitment to implement our professional values can weaken due to factors such as high levels of disabling workplace stress.
Three takeaway points about values in our practice:
♦ It is important that we often think about and reflect on our positive professional values because this strengthens our commitment to implement them in our practice.
♦ It is important that we also think about and reflect on negative values because this helps us to be aware of them and avoid implementing them in our practice to every possible extent.
♦ We must open ourselves to a very strong commitment to our positive professional values because this commitment enables us to face down and reject negative values and avoid implementing them.
► Now, what are values?
Values are powers we feel within us that motivate us; values and motivation go together.
A value-urge is like the current of a value's power as we feel the value within us.
An ensemble of value-urges is the combination of many different positive and negative value-urges that we experience within us that motivate our attitudes and activities. This ensemble can be likened to an orchestra made up of many different musical instruments. The instruments have different sounds which may be beautiful or harsh and which fluctuate in pitch and intensity as we feel them flow into one another and emerge from one another.
For example, we've all felt "the sound" of our professional value-urge of compassion as a power motivating us to respond immediately to an anguished or suffering patient and provide help and support.
Likewise, it's fair to say that we've all felt "the sound" of the negative value-urge of resentfulness as a power motivating us to get back at a patient or colleague who has been rude or treated us unjustly.
Thus, our motivation, the ensemble of value-urges which flow into one another and emerge from one another as we feel their power within us, will consist primarily of our positive professional values but is likely to also include negative values.
► Now, how do values work?
♦ .. As we feel the motivating powers of our ensemble of value-urges we simultaneously allow them to actually motivate us – when we accept them as ours – by truly valuing them.
♦ ..Then, the value-urges that we accept as ours by truly valuing them – invite us to follow them.
♦ ..We can choose to follow and implement the value-urges – or we can choose to pass them by and not implement them.
This process of how values work is not something we have to think about specifically as we practice. We can recognise this process as something we're already aware of but have not thought about before in this way.
Importantly, this process demonstrates to us that despite the level of motivating power of values, we choose which value-urges we truly value and accept as ours and which we don't truly value and don't accept as ours. Even for values we initially truly value and accept as ours, we can still choose whether or not to follow and implement them or to not follow and not implement them. We have control of our values-based practice.
Knowing what values are and how they work helps us better understand how we implement our professional nursing values and how we can avoid implementing negative values. Also, when others ask us about our nursing values we are able to explain what they are and how they work in our practice.
Scenario
The following scenario illustrates how Edith Stein's value theory guides our implementation of values. It is a hospital-based scenario written by a clinical nurse but can be generalised to any practice setting.
The circumstances of the hospital ward in which I practice are very stressful.
As I'm about to enter my ward I stop for 30 seconds, take some slow deep breaths and become aware of my ensemble of value-urges. I alert myself to feel the power current of my contagious calmness value-urge; I accept it as mine by truly valuing it, it invites me to follow it, and I absolutely commit myself to follow it and remain contagiously calm during my shift.
I enter my ward and receive the handover report. As I make my initial check with each of my group of 12 patients, I alert myself to feel the power of my watching-assessment-recognition value-urge; I accept it as mine by truly valuing it; it invites me to follow it; I do so with steadfast commitment because I know how vitally important it is to patient safety.
Among my group of patients is a man receiving chemotherapy to treat metastatic bone cancer. He is becoming increasingly restless because he is suffering from an increase in acute pain despite having received the maximum dose of his prescribed analgesic medication.
Amidst my ensemble of value-urges as I attend to my patient, I feel the power of my compassion value-urge; I accept it as mine by truly valuing it; it invites me to follow it and I choose to follow it. I immediately assess his analgesic regimen and consult with the pain management team to provide additional analgesia, which I administer to him. I initiate reassessment of his need for a more effective analgesic regimen.
Simultaneously, I also feel the power of my values-urges of attentiveness, kindness and gentleness which I accept as mine by truly valuing them; they invite me to follow them and I choose to follow them.
I implement these values by taking two minutes to attend with contagious calmness to my patient. I talk with him and touch him with kindness and in a gentle manner as I help him try to achieve a more comfortable physical position.
In my attentiveness to my patient, my two minutes are totally his in a way that I hope will stay with him after I leave him. Contagious calmness enables me to achieve this attentiveness, even though I know in the back of my mind that I have 11 other patients to attend to who also have a range of complex nursing needs.
As I turn toward the care of my other patients, I feel amidst my ensemble of value-urges the power of negative value-urges; anger with my hospital nursing department for frequent inadequate staffing of my ward, resentment toward my clinical nurse manager for remaining mostly in her office, seemingly detached from the pressures and stresses felt by myself and my clinical nursing colleagues, and appearing to accept as given the anguish some patients are experiencing.
I also feel the power of negative value-urges concerning myself and my nursing colleagues; fury with myself for not being able to provide the best possible care for all my patient group and finish my shift on time, and cowardice in relation to myself and my nursing colleagues for our not having the courage and perseverance needed to gain more control over our nursing practice and practice surroundings.
Nonetheless, as I head toward another of my patients, and check-in with the power current of my contagious calmness value-urge, I simultaneously don't allow my negative value-urges to motivate me by choosing not to accept them as mine, that is, by choosing not to value them.
Even if I do find myself valuing my negative value-urges by accepting them as mine, and they consequently invite me to follow them, I choose to pass them by; to not follow them and not implement them.
Consequently, I don't cast a resentful look at my clinical nurse manager as she glances up momentarily through her office window, and I don't start berating myself in my mind for not being able to provide the best possible care for my patients and finish my shift on time. I will persevere and encourage my nursing colleagues to persevere in our common aim to gain more control over our nursing practice and practice surroundings. And, come hell or high water, I will not give up my nursing profession.
I know that there are other constructive things I can do to address my negative value-urges. I also resolve to continue practicing "stillness" for at least five minutes every day during my personal time, the sure source of my contagious calmness value-urge power current.
In discussing her value theory, Edith Stein identifies factors that influence how our values work (Stein, 1921/1989; Lebech, 2015). The depth with which people feel particular types of value-urges depends on their personal disposition or personality.
A person's energy level influences how they implement values. A person may or may not feel strong enough to truly value the motivating power of professional values. Likewise, a person may or may not feel strong enough to resist the motivating power of negative values.
A person's level of commitment to the values they are responsible to implement, such as those of a profession, influences the perseverance with which their values are implemented under difficult circumstances
Summary
Given that values are the central stabilising element of PPMs, knowledge about values and their implementation in nursing practice is of central importance for the PPM of Careful Nursing. Edith Stein's value theory, used to define and understand Careful Nursing values, provides a definition of values and a framework for understanding their implementation in Careful Nursing practice.
Implementing the PPM of Careful Nursing
It is likely that you will recognise most of the PPM dimensions and their concepts because they are already part of your practice. We have always sought to create healing surroundings for patients and for ourselves. For many years we have followed 'the nursing process'. Careful Nursing follows the nursing process, but in more detail and in greater depth.
What the PPM of Careful Nursing does is organise, strengthen and deepen our understanding of the every-day essentials of our nursing knowledge and practice; it puts them into a 'mind map' or theoretical framework that we can use to routinely check on how we are doing in terms of the essentials of our practice.
The PPM guides us to consider the depth and complexity of the nursing process; it guides us to provide our distinctive nursing care for patients and document and measure its effectiveness while also undertaking a central role in the collaborative practice of the multidisciplinary team. At the same time, in some ways implementing the PPM can seem like a big change in how we practice; but this change can bring benefits such as increasing our control over our practice and giving us more time to spend with patients (Murphy et al. 2017).
Implementing the PPM: practice provisions
►As we consider implementation of each dimension of the PPM it is essential that we are guided by the Careful Nursing philosophical principles which describe who we are as human persons.
►In Careful Nursing we and all people we interact with are understood as human persons as described in the philosophical principles.
►Each human person is understood as a unique, individual body-spirit composite; each is unitary or holistic.
►Each person by definition has a spiritual essence which is intimately related to their mind or intellect.
►In accordance with their spiritual essence all persons possess inherent dignity, free will, and are predisposed to be loving and generous.
►Person-centred care in Careful Nursing is defined according to these practice provisions
'I will' statements: embedding the PPM concepts in clinical practice
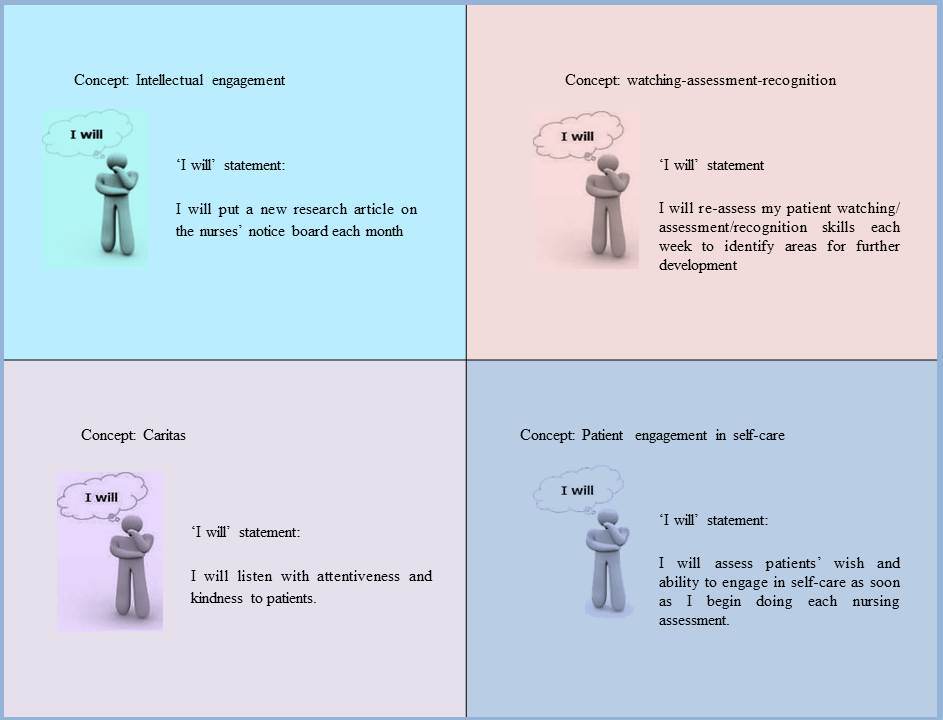
It is not always easy to change patterns of practice and it can take time to follow through on a new intention to do something in a particular way. Nurses learning about and implementing Careful Nursing in their practice have found this to be so. But, we have also found a solution, a practice embedding tool: creating and using 'I will' statements.
Using 'I will' statements originated with nurses at Mercy Hospital and Medical Center, Chicago, USA, When they first began learning about and implementing the preliminary model of Careful Nursing in 2006, they developed practical ways of transferring concepts into actions, one of which was developing 'I will' statements, that is, what they would actually do to implement each concept. To develop 'I will' statements the nurses worked together to think about and discuss each concept. Then for each concept, they agreed using their own words how they would express the concept in their practice attitudes and activities. They developed agreed upon attitudes and activities, or 'I will' statements for implementing each concept (Roemer 2006). They kept lists of their 'I will' statements in places such as on the backs of their name badges and on flip-cards for easy access and review at nurses-stations.
As the PPM of Careful Nursing has been implemented in other hospitals, 'I will' statements have been used. Here are some examples:
The PPM of Careful Nursing dimensions and concepts
In the following pages each dimension is described. For each dimension, in its sub-pages each of its concepts in described.
Acknowledgement
The author wishes to thank Dr. Mette Lebech, Department of Philosophy, Maynooth University, for her assistance in explaining Edith Stein's value theory and how it can be used to guide nursing practice.
References
American Nurses Credentialing Center (ANCN) (2014). Magnet Application Manual. ANCN, Silver Springs, MD
Hoffart N & Woods CQ (1996) Elements of a nursing professional practice model. Journal of Professional Nursing,12, 354-364.
Lebech, M. (2015) The Philosophy of Edith Stein. Peter Lang, Bern, Switzerland.
Murphy S, Mc Mullin R, Brennan S & Meehan TC (in press) Exploring implementation of the Careful Nursing Philosophy and Professional Practice Model© in hospital-based practice. Journal of Nursing Management.
Roemer J (2006) Reports on Careful Nursing to Senior Leadership Team and Nursing Division. Mercy Hospital and Medical Center, Chicago, USA.
Slatyer S, Coventry L, Twigg D & David S (2016) Professional practice models for nursing: a review of the literature and synthesis of key components. Journal of Nursing Management, 24, 139–150.
Stein, E. (1922/2000) Philosophy of Psychology and the Humanities. ICS Publications, Washington.
Therese C. Meehan © July 2020