In a nutshell . . . .
This page introduces you to the second of the six ideas that give life to the Therapeutic Milieu, Intellectual engagement. We often think in terms of the heart and hands of nursing, but this page proposes that it is in the mind of nursing that our greatest treasure is to be found – in our intellectual engagement.
It is intellectual engagement that alerts us to recognising the earliest possible early warning indicators of potential or actual physiological instability in patients – it is key to patient safety.
But, in our focus on the actual doing of nursing, often under very pressured circumstances, the lightning-quick capacity of our mind to understand, arrange and direct everything we do can slip below our level of awareness.
Sometimes we may even think that we are not intellectual, thanks to memories of struggles with term papers and exams. But, Careful Nursing says not to let such memories get the better of you. As human persons we all have abundant capacity for intellectual engagement. There is nothing that is beyond the reach of our mind.
In this page you will read about intellectual engagement in clinical practice, critical thinking and evidence-based practice, and experience and intuition as ways of knowing. You will find steps to follow to "get a grip" on reading and understanding research reports and other academic articles. You will also find easy-to-follow steps for critical thinking and critical reading, and guidelines for debating nursing ideas.
The Careful Nursing message about intellectual engagement is two-fold; it is critical to patient safety – and can lead to lots of Aha! moments and be lots of fun.
Introduction
Intellectual engagement is the second concept of the Therapeutic Milieu because the inner spirituality and intellect of the human person are intimately interrelated. Through our intellect, or mind, we are intimately linked to the first principle of our being, as outlined in the Careful Nursing philosophy page on the nature and inherent dignity of the human person. Our mind, our thinking, our intellectual engagement, is a primary principle of our practice as professional nurses.
For Careful Nursing intellectual engagement has been defined as 'Nurses' ability to conceptualise, think creatively and critically, and theorise about nursing practice using nursing and other related knowledge and to do this in relation to knowledge of the social, political and economic context of their practice. . . . it includes using contemplation and empathy as well as natural reason, logical analysis and scientific research to guide, implement and evaluate nursing practice and health care. (Meehan 2012, p. 2910). We can also include philosophical thinking in this definition.
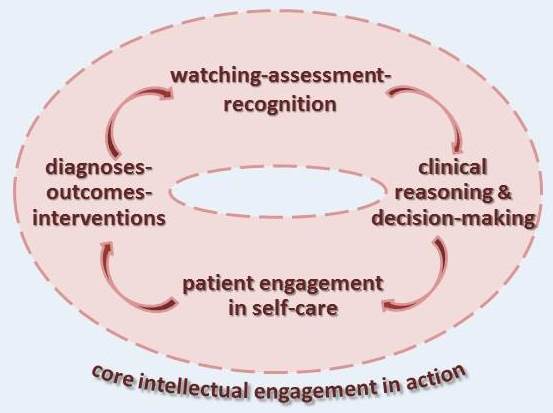
Intellectual engagement in clinical practiceIn Careful Nursing intellectual engagement permeates implementation of all concepts of the professional practice model, especially watching-assessment-recognition, clinical reasoning and decision-making, patient engagement in self-care and diagnoses-outcomes-interventions. In practice, intellectual engagement is the knowing that guides our doing.
Intellectual engagement requires that we question our day-to-day practice, that we are ever mindful of the knowledge that is guiding our practice, of the actual best-evidence that underlies our practice. It requires that we keep up with the latest nursing literature, for example, that we read a study or article about an aspect of our practice at least once a month and share what we learn with colleagues.
Intellectual engagement also includes keeping a pocket-size notebook to hand in which we can jot down questions and ideas that occur to us as we practice and experiences that we have, so we can think about them later. We could compare our questions, ideas and experiences to the literature and think about and begin writing about them ourselves.
However, in our day-to-day practice, as we face the challenged to do as much as possible, it is all too easy to let our habit of intellectual engagement fade. Also, we may overlook how nimbly our mind choreographs our myriad of sense impressions, streaming them to our imagination, memory, and reasoning power to provide the rich ground for our insight, understanding, knowledge, judgements, attitudes and activities.
Sometimes we might even think we are not intellectual because we associate thinking with struggles with term papers and examinations. But, intellectual engagement is not only an ability; it is a property which we all have, potentially and actually and in abundance. Thinking and understanding has many dimensions and there is nothing that is beyond the reach of our mind (Aquinas 1265-1274/1948, I, Q. 84-87).
Two types of intellectual engagement that are ever-present in our practice are evidence-based practice and the combination of experience and intuition.
Critical thinking and evidence-based practice
Foremost in our mind as we practice is the importance of critical thinking and evidence-based practice. Evidence-based practice originated in medicine and developed in nursing from emphasis on research utilisation. Evidence-based practice broadened research utilisation to encompass use of the best available evidence in caring for patients according to their individual needs and circumstances (Beyea & Slattery 2013). An early medical definition of evidence-based practice remains the most true to its meaning: 'conscientious, explicit and judicious use of the best evidence in making decisions about the care of individual patients (Sackett et al.1996, p. 71).
Sackett et al. (1996) emphasise that evidence-based practice is based on a combination of clinical expertise and best available evidence; when scientific evidence is not available, the next best available evidence is used. Dogherty et al. (2010) observe that evidence-based practice can be facilitated by individual nurses or groups of nurses, that leadership and management are important in its implementation, and importantly that 'tailoring facilitation to the local context is critical' (p. 76).
Evidence-based practice is incorporated in Careful Nursing particularly through use of the mostly evidence-based standardised nursing languages of NANDA-I™ nursing diagnoses (Herdman & Kamitsuru 2014), nursing outcomes classification (NOC) (Moorhead et al. 2013) and nursing interventions classification (NIC) (Bulechek et al. 2013), which are used to construct patient nursing care plans.
Use of this care planning system can most clearly illustrate nurses' natural intellectual engagement as they assess and re-assess patients using diagnoses' defining characteristics and related factors to make and revise nursing diagnoses as necessary, and as they measure nursing outcomes (Murphy et al. 2017).
Gradually, an evidence base is being identified for all the professional practice model concepts; for example, by identifying evidence that supports the nature and effectiveness of the nurse-patient relationship (Conroy et al. 2017) and approaches to clinical reasoning and decision-making (Price et al. 2017).
Experience and intuition
In addition to using objective ways of reasoning, we use a multiplicity of subjective ways of reasoning, particularly intuition. In a concept analysis of intuition in clinical nursing practice, Robert, et al, (2014) conclude that many nurses experience intuition spontaneously and use it in clinical reasoning. A unitary approach to practice, as is used in Careful Nursing, can provide insight into the nature of intuition and also support our use of other experiential types of clinical reasoning, such as narrative and aesthetic reasoning.
Writing in the tradition of Aquinas, the philosopher Maritain (1953) argues that a natural, semi-conscious, intuitive reasoning is deeply embedded in human persons and sees with an 'intuitive grasping' which gives rise to analogical reasoning and also forms the foundation for logical reasoning (p. 75). Green (2012) provides a detailed discussion and analysis of neurophysiological research and philosophical arguments, drawn partly on the work of Maritain, which support nurses' use of intuition as a valid form of knowledge in practice.
Engaging with the nursing literature and debating ideasIt goes without saying that intellectual engagement is essential for critical reading and thinking and that critical thinking is essential for skilled, evidence-based practice. Intellectual engagement means reading professional literature; critically reading the research literature and being familiar with the most recent research findings related to our practice and using research findings to guide our practice. It also means reading and analysing nursing theories, frameworks and models, and related literature from other disciplines.
How to 'get a grip' on a research report or discursive article
Here the term 'get a grip' means to have a newfound understanding of a topic or concept, for example, realising that a research report is actually not that difficult to read; or to control one's reactions or emotions, for example, to overcome any feelings of apprehension or hopelessness at the sight of descriptive or inferential statistics.
Probably one of the best nursing research texts available is Nursing Research: Methods and Critical Appraisal for Evidence-Based Practice by LoBiondo-Wood and Haber (2017); ideally every practicing nurse would be able to read this book with great interest. However, nurses who received their undergraduate education in one of the many countries where undergraduate nursing education still does not include a dedicated nursing research module and a dedicated beginning statistics module are likely to find this book challenging to read and understand.
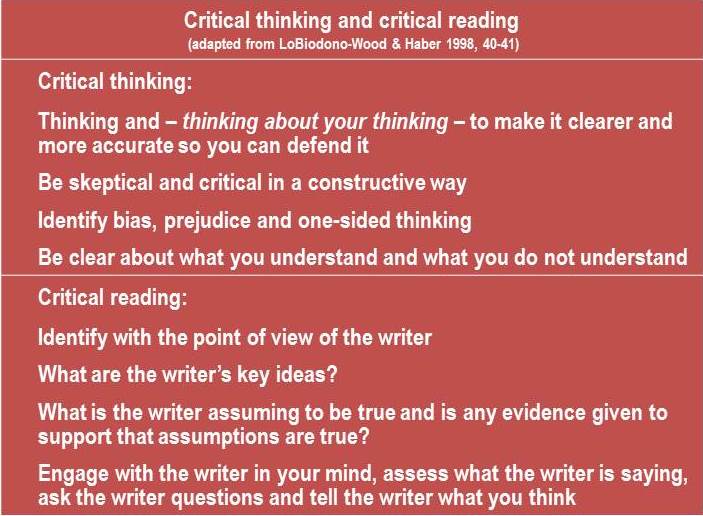
To begin with, earlier editions of the LoBiondo-Wood and Haber book may be most useful for getting a grip on how to read and understand research and other nursing articles. In earlier editions, for example, Nursing Research: Methods, Critical Appraisal, and Utilization, LoBiondo-Wood and Haber (1998), these authors discuss the nature of critical thinking and critical reading; they suggest a practical and engaging approach to intellectual engagement. You are encouraged to read the original (pp. 40-41), a summary of which is shown in the following Table.
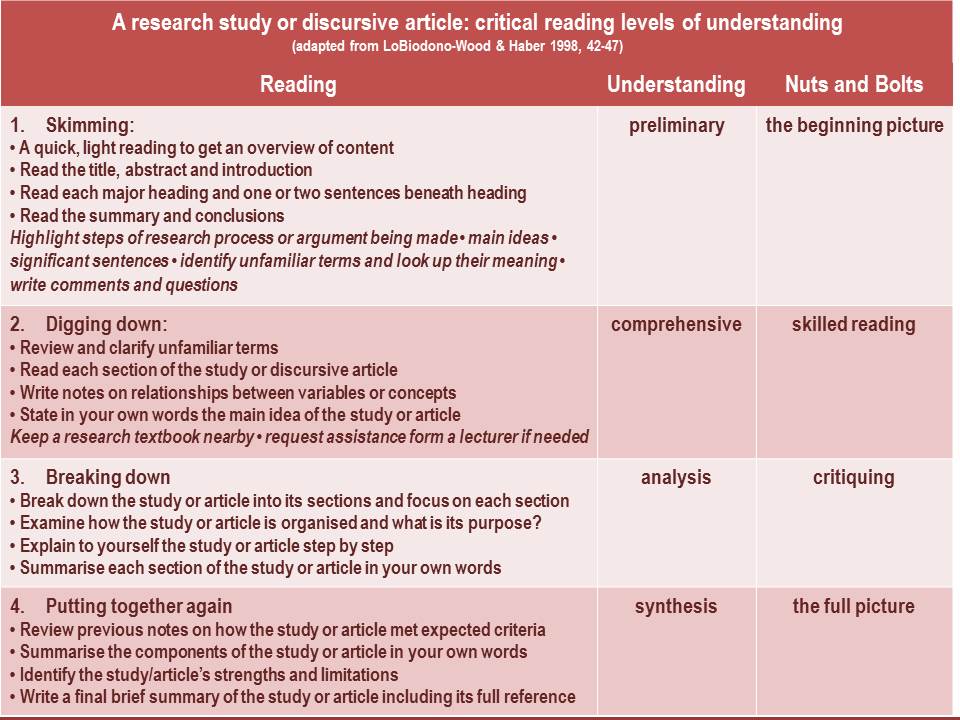
LoBiondo-Wood and Haber (1998) also present and discuss a four-level strategy for critically reading and understanding research reports. These four levels of reading and understanding can be used for any professional article, whether it is a research report or a discussion and analysis of a theory, framework, concept or procedure.
An advantage of the four-level LoBiondo-Wood and Haber (1998) strategy is that it makes a research report or discursive article relatively easy to read; in the mind of the reader it 'cuts it down to size'. For example, in doing the first level of the strategy, skimming, the reader is guided to quickly get an overall appreciation of a study or article so that reading it again in more depth becomes something you feel drawn into doing; one level of reading draws you naturally to the following level so that you finish with a good grip on the study or article. You are strongly encouraged to read the presentation and discussion of the four-level strategy (pp. 42-47), a summary of which is shown in the following Table.
How to debate ideas: disputation for decision-making
Before the rise of science, and developing in the first universities in the 12th century, the hallmark of intellectual engagement and critical thinking was a formal academic disputation (Novikoff 2013). Simply put, an academic disputation is a debate; a method of knowledge development using argument for and against a topic; it seeks to eliminate error and biased thinking, and determine as closely as possible what is true about the topic. Argument remains the method of knowledge development used in philosophy. A disputation can be very effective in verifying ideas for making evidence-based decisions.
Disputations were originally conducted in person as academic lectures but were also presented in written form. All arguments made in a disputation had to be supported by referenced literature. At the completion of a disputation the writer would aim to have rejected convincingly all possible arguments refuting the truth of the original proposition about the topic. Only when arguments refuting the proposition could be convincingly rejected, could the proposition be accepted as probably true.
Aquinas is recognized as a master of disputation (Novikoff 2013); if you read the Summa Theologica by Aquinas (1265-1274/2007) you will notice right away that all the topics and questions are addressed and 'proved' using the disputations method.
Disputation is a great way to develop critical thinking skills. It can be adapted easily to writing a term paper, structuring a seminar or exploring any clinical practice topic. For example, imagine that you are asked to write a term paper discussing use of nursing professional practice models in hospitals. You could begin with the proposition that use of a professional practice model is an effective approach to structuring nursing practice in hospitals. Then you would state your proposition as a question: Is use of a professional practice model . . . ? Then you would propose a negative response to your question: Professional practice models are not effective . . . . Then you would develop four or five arguments, supported by the literature, that professional practice models are the models of not effective. Here now is the challenge to biased thinking, error and personal opinion. You must face up to and explore the reasons your proposition may be wrong. And, this is only the beginning.
The format and an example of a disputation, using a Careful Nursing assumption as the topic, are shown in the Table below. You could use it as a model for critically exploring and analysing your own topic.
MethodExample Using a Careful Nursing AssumptionFormulate a reasoned assumptionThe philosophy of Aquinas is an appropriate philosophical foundation for Careful Nursing.State the assumption as a questionIs the philosophy of Aquinas an appropriate philosophical foundation for Careful Nursing?Propose a negative response to the questionIt seems that the philosophy of Aquinas is not an appropriate philosophical foundation for Careful Nursing.State 3–5 objections in support of the negative response to the questionObjection 1: Aquinas was a Christian theologian as well as a philosopher and almost everything he wrote was shaped by his theology (Floyd, 2010). Aquinas's religious views compromised his ability to truly engage in philosophical debate and his philosophy amounts to little more than special pleading for his own personal point of view (Russell (1945/1972). Therefore, the philosophy of Aquinas is not an appropriate philosophical foundation for Careful Nursing.Objection 2: Scholarship based on the philosophy of 13th century thinkers is unreliable because only a small number of their texts have been cataloged and few have been translated from Latin into modern languages. Specialized knowledge of the historical period is necessary for their valid interpretation for contemporary application (MacDonald & Kretzmann, 1998). Therefore, the philosophy of Aquinas is not an appropriate philosophical foundation for Careful Nursing.
Objection 3: Contemporary nursing knowledge development is a scientific endeavor and models and theories of nursing are founded on advanced, post-Enlightenment, thinking (Fawcett & DeSanto-Madeya, 2012). A comprehensive presentation of philosophies relevant to nursing knowledge development (Rogers 2005) includes ancient philosophers up to Aristotle and then continues directly to Descartes, indicating that philosophers of the 1,700-year intervening period are not relevant to nursing. Therefore, the philosophy of Aquinas is not an appropriate philosophical foundation for Careful Nursing.
Objection 4: "Real nurses nursing real patients are busy and tired, and therefore unable to engage in elaborate conceptual exercises throughout their working day" (Newton, 1991, p. 193). Thus, there is no point in encouraging nurses in practice to think philosophically about the nature of their patients, themselves, and their practice. Textbooks on nursing models and theories address philosophy of science but pay minimal attention to philosophy of nursing per se (McKenna et al, 2014). Therefore no philosophy, including that of Aquinas, is an appropriate foundation for Careful Nursing. Make a statement contrary to the objections (a positive response to the question)On the contrary: Philosophy from the 13th century period offers rich resources for the development of contemporary philosophy (Koterski, 2009). A widely recognized present-day philosopher Alasdair MacIntyre (2007, 2009) reasons that the ideas and arguments developed by Aquinas are of vital importance in understanding the nature of human beings and the ethics of the social, political and economic activities which they create; all of which are of central importance to nursing's concern with human health and flourishing.State your own reasoned response to the question as a concise discussionI respond that: According to the etymological origin of the term nurse (Connell, 1983) and the documented public service provided by nurses since the 1st century C.E. (Meehan, 2012b), the purpose of nursing is the nurturance and protection of sick, injured and vulnerable human beings and fostering of their health. The profession's claim to view the human being as a unitary (holistic), spiritual being is well established in contemporary professional literature (Alligood & Marriner-Tomey, 2010). But, comprehensive philosophical foundations that support these claims is generally absent (Sarter, 1988), or limited to so-called world views constructed from concepts of contemporary science and philosophies of science (Fawcett & DeSanto-Madeya, 2012). This situation exists because universities tend to be dominated by Cartesian, scientific thinking to the detriment of human sciences and exploration of pre-Enlightenment philosophical thought (Scruton 2004). Universities also generally avoid exploration of the spiritual dimension of human life from any particular Western philosophical perspective (MacIntyre, 2009; Scruton, 2015). Thus, contemporary nurses have tended to be cut adrift intellectually from philosophies deeply consistent with descriptions and explanations of nursing. Likewise, they have tended to lose their professional historical consciousness and until recently their spiritual consciousness. The philosophy of Aquinas addresses ideas of great importance to nursing in depth and detail, providing an abundant source of propositions and theories for the nursing profession to drawn on.Reply to each objection explaining why it is incorrect or inadequate.Reply to objection 1: Although Aquinas was a Christian theologian as well as a philosopher, his thinking and conclusions were developed strictly according to objective, reasoned argument. Much of his writing is based on the work of Aristotle and regarded as philosophical. Formerly, theology and philosophy were so interrelated that even some of Aristotle's philosophical writing is considered theological (McInerny & O'Callaghan, 2015). Aquinas was meticulous in distinguishing between his thinking as a theologian and his thinking as a philosopher (Kenny, 2002).
Reply to objection 2: Scholarship from the 13th century is voluminous because universities were just beginning to develop at that time. While much of this scholarship is available only to specialists, the writings of Aquinas are an exception. Almost all his extensive writings have been translated from Latin into modern languages by different translators. His writings and the translations are widely verified, commented on and discussed in relation to his historical period (Thomas Instituutte Utrecht , 2002).
Reply to objection 3: Despite bias in the nursing profession for scientific approaches to knowledge development by theorists (Fawcett & DeSanto-Madeya, 2012) and philosophers (Rogers, 2005), nurses in practice seek humane approaches to understanding the unitary, spiritual nature of patients (McGee, 2000). Watson's caring science (Sitzman & Watson, 2014) responds to this need but explains the spiritual and holism in nursing by drawing on popular Eastern philosophies such as Buddhism and by using Western pre-Enlightenment terms lifted out of their original context and redefined, for example caritas.
Reply to objection 4: A hallmark of professional practice is to be intellectually engaged. Any claim by nurses that they are too busy and too tired to think about what they are doing is incompatible with professional responsibility. Nurse–philosophers are becoming more concerned with development of philosophical approaches to practice as they think they will contribute to understanding practice beyond concerns with technical expertise and measurable outcomes (Holt, 2013).
Intellectual engagement 'I will' statements
Sit quietly in a chair, close your eyes and take a moment to relax and recall your experience of stillness. Bring to mind your practice experiences over the past three months.
On a scale of 1 to 10, how do you rate your intellectual engagement?
 Based on your assessment of your current level of intellectual engagement, decide what will you do to strengthen and deepen your intellectual engagement as you practice?
Based on your assessment of your current level of intellectual engagement, decide what will you do to strengthen and deepen your intellectual engagement as you practice?
Examples of nurses' intellectual engagement 'I will' statements:
. . . keep myself up to date by reading two nursing articles each month
. . . share new information I have learned with my colleagues
. . . complete a nursing professional development course online every year
. . . . . . . . . . . . . . . . . . . . . . . . .find a nursing journal I like to read regularly
ReferencesAquinas T (1265-1274/2007) Summa Theologiae. Cambridge University Press, Cambridge.
Beyea SC & Slattery MJ (2013) Historical perspectives on evidence-based nursing. Nursing Science Quarterly,26, 152–155.
Bulechek GM, Butcher HK, Dochterman JM & Wagner C. (eds.) (2013) Nursing Interventions Classification (NIC), 6th edn. Mosby, St. Louis.
Conroy T, Feo R, Boucaut R, Alderman J & Kitson A (2017)Role of effective nurse-patient relationships in enhancing patient safety. Nursing Standard, 31, 53-63.
Dogherty EJ, Harrison MB & Graham ID (2010) Facilitation as a role and process in achieving evidence-based practice in nursing: A focused review of concept and meaning Worldviews on Evidence-Based Nursing, 7, 776–89.
Green C (2012) Nursing intuition: a valid form of knowledge. Nursing Philosophy, 13, 98–111.
Herdman TH & Kamitsuru S (eds.) (2014) Nursing Diagnoses Definitions and Classifications 2015-2017. Wiley Blackwell, Oxford.
Novikoff AJ (2013) The Medieval Culture of Disputation: Pedagogy, Practice, and Performance. University of Pennsylvania Press, Philadelphia.
LoBiondo-Wood G & Haber J (1998) Nursing Research: Methods, Critical Appraisal, and Utilization (4th ed). Mosby, St. Louis.
LoBiondo-Wood G & Haber J (2014) Nursing Research: Methods and Critical Appraisal for Evidence-Based Practice (9th ed). Elsevier, St. Louis.
Maritain J (1953) Creative Intuition in Art and Poetry. Pantheon Books New York.
Moorhead S, Johnson M, Maas M & Swanson E (2013) Nursing Outcomes Classification (NOC), 5th edn. Mosby, St. Louis.
Meehan T C (2012) The Careful Nursing philosophy and professional practice model. Journal of Clinical Nursing, 21, 2905–2916.
Murphy S, Mc Mullin R, Brennan S & Meehan TC (2018) Exploring implementation of the Careful Nursing Philosophy and Professional Practice Model© in hospital-based practice. Journal of Nursing Management, 27, 2260-2273.
Price A, Zulkosky K, Wite K & Pretz J (2017) Accuracy of intuition in clinical decision-making among novice clinicians. Journal of Advanced Nursing, 73, 1147–1157.
Robert RR, Tilley DS & Petersen S (2014) A power in clinical nursing practice: concept analysis on nursing intuition. Medsurg Nursing, 23, 343-349.
Sackett DL, Rosenberg WMC, Haynes RB & Richardson WS (1996) Evidence-based medicine: What it is and what it isn't. British Medical Journal, 312, 71.
Therese C. Meehan© July 2020